Maxillary canine‒second molar transposition: A rare case report
J Dent Res Dent Clin Dent Prospects, 11(2), 131-134; DOI:10.15171/joddd.2017.024
Clinical Dentistry
Maxillary canine‒second molar transposition: A rare case report
Somayeh Hekmatfar1, Karim Jafari2*, Firoz Zadfatah3, Sahar Mousavi2
1
Department of Pediatric Dentistry, Dental Faculty, Ardabil University of Medical Sciences, Ardabil, Iran
2
Department of Prosthodontics, Dental Faculty, Ardabil University of Medical Sciences, Ardabil, Iran
3
Department of Endodontics, Dental Faculty, Ardabil University of Medical Sciences, Ardabil, Iran
*Corresponding Author; Email: ddsjfr@gmail.com
© 2017 by Tabriz University of Medical Sciences
Abstract
Tooth transposition, which is a rare condition, is ascribed to the disturbance of tooth eruption and the subsequent abnormal occlusal relationships. Transpositions mostly involve the upper jaw and more frequently occur between the maxillary canine and first premolar. Herein, we present a case of a maxillary canine‒second molar transposition in a thalassemic patient.
Keywords: Maxillary canine, transposition, thalassemia
© 2017 Hekmatfar et al. This is an Open Access article published and distributed by Tabriz University of Medical Sciences under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Tooth transposition is a rare condition, which refers to the disturbance of tooth eruption and the subsequent abnormal occlusal relationships.1 The incidence rate of this condition differs based on the sample studied; however, in the majority of the case studies, this rate has been reported to be under 1%.2-4 Transpositions mostly involve the upper jaw and are more frequently seen between the maxillary canine and first premolar.5-6 Canine transposition mostly occurs in the females.6-7
Peck and Peck categorized the maxillary transposition into five types, arranged by incidence, including canine‒first premolar, canine‒lateral incisor, canine‒first molar, lateral incisor‒central incisor, and canine‒central incisor.6 The canine transposition is a multifactorial condition, which is associated with both genetic and environmental factors.8 Several risk factors have been identified for this dental anomaly, including the positional interchange of tooth buds,7-9 deviation from the normal eruption path,10 existing primary teeth,11 and trauma.12 In addition, some medical conditions and systemic diseases, such as blood dyscrasia, may lead to this condition.
Fanconi anemia is a rare genetic disease caused by decreased blood cells, which affects the bone marrow. This disease is associated with dental anomalies. According to Goswami et al, microdontia, supernumerary teeth, tooth agenesis, discolored teeth, abnormal tooth shape, rotation, transposition and delayed eruption are among the most common dental anomalies observed in patients with Fanconi anemia.13 Tekcicek et al24 reported that transposition occurred in 9% of the children with Fanconi anemia.
Thalassemia is a hereditary chronic microcytic anemia described by deficiency in hemoglobin synthesis and ineffective erythropoiesis. This disease is one of the most confusing hemoglobinopathies.14 According to Khojastehpour et al, dental anomalies are more common in thalassemic patients than in normal individuals. The aim of this paper is to report a case of a maxillary canine‒second molar transposition in a thalassemic patient.
Case report
A 22-year-old woman referred to the Ardabil Dental Faculty Clinic, Ardebil, Iran, with a chief complaint of pain in the upper first molar area. The patients’ medical history revealed that she was a known case of β-thalassemia minor. She had undergone splenectomy five years ago without any history of blood transfusion. Due to high platelet counts, aspirin was recommended by an oncologist to reduce the risk of thromboembolism.
The intraoral examination revealed the transposition of the left maxillary canine that erupted mesial to the third molar (Figure 1). The distal slope of the canine was in contact with the mesial marginal ridge of the lower left third molar. The crown of the transpositioned canine was well-formed with a prominent cingulum (Figure 2).

Figure 1. Intraoral view of the canine erupting mesial to the third molar.

Figure 2.Occlusal view of the transposed maxillary canine.
The left maxillary first and second molars as well as the right and left mandibular first and second molars were missing. Furthermore, major occlusal plane discrepancies were observed due to the mandibular posterior teeth lost. The right canine was also missing. The patient interview revealed that the mentioned tooth was impacted and already surgically extracted by an oral and maxillofacial surgeon. The upper and lower dental midlines did not coincide, and there were spaces between the lower anterior teeth.
The right and left deciduous maxillary canines were retained. The rare occasional finding in this patient was the transposition of the left canine that erupted mesial to the third molar (Figure 1). The left first and second molars were absent. The patient did not remember anything about these teeth.
The patient underwent radiological examination. The panoramic views revealed the enlargement of marrow spaces with widened trabeculae in both the maxilla and mandible (Figure 2). The soft tissue drapes had normal color and contours. The only abnormal finding in soft tissue examination was macroglossia (Figure 4).

Figure 3.Panoramic view of the enlargement of marrow spaces with widened trabeculae.
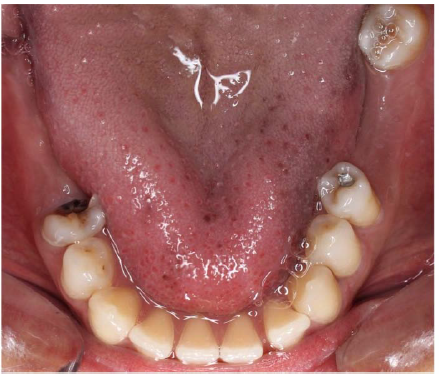
Figure 4. Macroglossia in a thalassemic patient.
To determine an appropriate treatment plan, an impression was made of both dental arches. The stone casts were mounted on a semi-adjustable articulator by the means of a facebow. The analysis of the mounted casts showed a severe occlusal plane discrepancy as well as over-erupted right second premolar and first molar that had contact with the lower edentulous ridge.
In this condition, the prosthodontic treatment modality necessitates administration of extensive orthodontic and surgical interventions to create adequate space for the replacement of the missing tooth. However, due to economic issues, the patient did not accept any prosthodontic treatment and only received endodontic therapy for the maxillary first molar.
Discussion
Tooth transposition is a form of ectopic eruption, which can affect the maxillary or mandibular arch. This dental anomaly frequently involves the canine and first upper premolar.5-6 The unilateral dental transpositions are more prevalent than the bilateral ones and mostly affect the left side.1,5 No transposition has been reported in the deciduous dentition yet.5,13
Tooth transposition can be complete and incomplete based on the position of the roots and the crowns of transposed teeth. While the complete transposition denotes the involvement of both the crown and root in the transposed position, the incomplete type represents the transposition of either the crown or the root apices.5 According to Peck’s classification (1995), there are five types of tooth transposition, depending on the teeth involved.6
In our case, we observed a complete transposition of the left maxillary canine, which was reported to have a high incidence in previous studies. However, regarding the study by Peck, the canine‒second molar transposition has not been reported in the literature. In a study conducted by Shanmugasundaram, the canine was reported to erupt buccal to the contact area between the left second premolar and the first molar.15 Furthermore, Kayipmaz reported a case of a 21-year-old man with a left maxillary canine‒molar transposition.
β-thalassemia is due to the diversity of genetic defects resulting in diverse hematologic and clinical features such as anemia. There are several different genotypes that may present similar clinical manifestations. Accordingly, Margot reported such manifestations as generalized rarefaction of the alveolar bone, thinning of cortical bone, “chicken-wire” appearance of the widened bone marrow spaces, and large trabeculae in radiographic examinations.23 We also observed the enlargement of marrow spaces with widened trabeculae in both the maxilla and mandible. Other dental anomalies, which may occur along with tooth transposition, include agenesis or malformation of lateral incisors and the retention of deciduous teeth.14
In our case, the primary canines were retained on the left and right sides. The permanent canine of the left side erupted in transposed position, and the canine on the contralateral side was surgically extracted. The maxillary lateral incisors were normal in size and shape. Tooth transposition is a multifactorial condition, which occurs as a result of environmental and genetic factors with complex relationships.8
The administration of radiography is a critical measure in the early diagnosis of tooth transposition, which can greatly affect prevention of eruption disturbances. Depending on the position of the tooth, it can erupt in an ectopic position or remain impacted. In our case, an early intervention could prevent the impaction of the right maxillary canine.
Two therapeutic approaches have been proposed for the management of transposition, namely interceptive and definitive treatment. The decision-making on transposition treatment depends on the time of diagnosis of this condition.6,15 The interceptive treatment can be carried out on the patients within 6‒8 years of age prior to the completion of transposition. The corrective measures for the eruptive path of the upper canines include extraction of retained deciduous teeth, positioning of the permanent lateral incisor in its physiological position, and maintenance of the space for the permanent canine.15,16
On the other hand, the definitive treatment consists of three phases, namely the extraction of one of the transposed teeth, alignment of the teeth in the transposed and correct position, as well as orthodontic correction.17,18
Conclusion
The dental management of medically compromised patients, such as those with thalassemia, needs special attention. Therefore, it seems essential to employ a multidisciplinary approach involving a dental surgeon, a hematologist, an orthodontist, and a prosthodontist to safely provide these patients with seemingly benign blood dyscrasia with dental treatment. Nevertheless, many factors may affect the treatment outcomes, including esthetics, occlusion, dental crowding, treatment period, patient motivation and cooperation, as well as periodontal support of the transposed teeth.1
Acknowledgments
The authors would like to thank the Vice Chancellor for Research Affairs of Dental Faculty of Ardabil University of Medical Sciences for their support.
Authors’ contributions
KJ and SH performed the radiographic and clinical examinations as well as the literature review. SH drafted the manuscript and prepared the figures. FZ and SM critically revised the manuscript. All authors read and approved the final manuscript.
Funding
The study was self funded.
Competing interests
The authors declare no competing interests with regards to the authorship and/or publication of this article.
Ethics approval
Patient reported in the study have given signed written consents for use of the photographs.
References
- Moschos A. Prevalence of Tooth Transposition A Meta-Analysis. Angle Orthod 2010;80(2):275-285.
- Ruprecht A, Batniji S, El-Neweihi E. The incidence of transposition of teeth in dental patients. J Pedod 1985;9:244–249.
- Sandham A, Harvie H. Ectopic eruption of the maxillary canine resulting in transposition with adjacent teeth. Tandlaegebladet 1985;89:9–11.
-
Burnett SE. Prevalence of maxillary canine-first premolar transposition in a composite African sample. Angle Or-thod.1999;69:187–189.
- Shapira Y, Kuftinec MM. Tooth Trasposition—a review of the literature and treatment considerations. Angle Or-thod.1989;59:271–276.
- Peck S, Peck L. Classification of maxillary tooth transpositions. Am J Orthod Dentofacial Orthop 1995;107:505–517.
- Peck S, Peck L, Kataja M. Mandibular lateral incisor-canine transposition, concomitant dental anomalies, and genetic control. Angle Orthod 1998;68:455–466.
- Ely NJ, Sherriff M, Cobourne MT. Dental transposition asa disorder of genetic origin. Eur J Orthod 2006;28:145–151.doi: http://dx.doi.org/10.1093/ejo/cji092. [Crossref]
- Peck L, Peck S, Attia Y. Maxillary canine-first premolar transposition, associated dental anomalies and genetic basis. Angle Orthod 1993;63:99–109; discussion 110.
- Gholston LR, Williams PR. Bilateral transposition of maxillarycanines and lateral incisors: a rare condition. ASDC J Dent Child 1984;51:58–63.
- Laptook T, Silling G. Canine transposition—approaches to treatment. J Am Dent Assoc 1983;107:746–748.
- Dayal PK, Shodhan KH, Dave CJ. Transposition of canine with traumatic etiology. J Indian Dent Assoc 1983;55:283–285.
- Goswami et al. dental perspective of Rare disease of Fanconi anemia: Case Report with Review. Clinical Medicine Insights: Case Reports2016:9 25–30.
- Saks hi Madhok. Dental considerations in Thalassemic patients. IOSR Journal of Dental and Medical Sciences 2014;13:57-62.
- Shanmuhasuntharam P1, Thong YL. Extreme distal migration of a maxillarycanine.Br Dent J. 1990 Jan 20;168(2):73-4.
- Kayipmaz, S., Saricaoğlu, S.T. &Sezgin, Ö.S. Unusual teeth transpositions: two case reports Oral Radiol (2009) 25: 81.
- Shapira Y, Kuftinec MM. Orthodontic management of mandibular canine incisor transposition. Am J Orthod 1983;83:271–6.
- Budai M, Ficzere I, Gabris K, Tarjan I. Frequency of transposition and its treatment at the Department of Orthodontics of Semmelweis University in the last five years. FogorvSz 2003;96:21e 24.
- Plunkett DJ, Dysart PS, Kardos TB, Herbison GP. A study of transposed canines in a sample of orthodontic patients.Br J Orthod 1998;25:203–8.
-
Plunkett DJ, Dysart PS, Kardos TB, Herbison GP. A study of transposed canines in a sample of orthodontic patients.Br J Orthod. 1998;25:203–8.
- Shapira Y, Kuftinec MM. Maxillary tooth transpositions: characteristic features and accompanying dental anomalies. Am J Orthod Dentofac Orthop.2001;119:127–34.doi: http://dx.doi.org/10.1067/mod.2001.111223.[Crossref]
- Shapira Y, Kuftinec MM. Maxillary canine–lateral incisor transposition? Orthodontic management. Am J Orthod Den-tofac Orthop 1989;95:439–44.
- Bennett JC, McLaughlin RP. Orthodontic management of the dentition with the preadjusted appliance. London: Mosby; 2001. p. 153-90.
- Margot L. Van Dis Thethalassemias: Oral manifestations and complications. Oral Surc. Oral Med. Oral Pathol 1986;62:229-233.
- Tekcicek M1, Tavil B, Cakar A, Pinar A, Unal S, Gumruk F. Oral and dental findings in children with Fanconi anemia. Pediatr Dent 2007;29(3):248-52.