A single-visit feeding plate for a 3-month-old infant with cleft
palate: A case report
J Dent Res Dent Clin Dent Prospects, 11(4), 253-256; DOI:10.15171/joddd.2017.044
Clinical Dentistry
A single-visit feeding plate for a 3-month-old infant with cleft
palate: A case report
Amro Mohammed Moness Ali ,1*, Abdullah Kamel2
1
Lecturer of Paediatric and Community Dentistry, Paediatric and Community Dentistry Department- Faculty of Dentistry Mania University Egypt
2
Assistant Lecturer of Prosthetic Dentistry Prosthetic Dentistry Department Faculty of Dentistry Mania University-Egypt
*Corresponding Author; Email: amromoness@mu.edu.eg
© 2017 by Tabriz University of Medical Sciences
Abstract
Infants with cleft palate (CP) have several problems, one of which is feeding, preventing the infant from maintaining adequate
nutrition. Use of a feeding plate, consisting of a special bottle and nipple, has been described to overcome this problem.
This article describes the steps of constructing a single-visit feeding plate for a CP infant. The main objective was to
provide an infant with a properly functioning feeding prosthesis and to reduce the parents’ anxiety originating from multiple
dental visits. We can conclude that our feeding plate successfully achieved the planned objectives.
Keywords: Feeding, hard palate,obturators, soft palate
Introduction
Cleft lip and palate (CL/P) is one of the most common congenital orofacial anomalies.1 Classification, possible etiological factors, pathogenesis and different management protocols of cleft palate have been described in the literature.2 Such cases require collaborative efforts by many specialists, among them a pedodontist and a prosthodontist to participate actively and efficiently.3,4 Feeding process in a CL/P child is usually difficult and feeding time is very long and both the infant and mother get exhausted.5
A feeding plate is not only critical for proper nutrition but also it has a role in craniofacial growth and reduces the incidence of otitis media and nasopharyngeal infections as well.6
Case report
A 3-month-old female infant, with non-contributory medical and family history, was referred to the Paediatric Dentistry Outpatient Clinic, Minia University Dental Hospital, Minia, Egypt, with a chief complaint of difficulty in feeding and nasal discharge. The mother reported that the infant was not able to suckle milk properly even with the use of typical cleft nipples or squeezable bottles and the infant was not gaining proper weight (only 7 pounds). There was no history of previous treatment or surgery for the defect. Intraoral examination revealed a cleft in the uvula, soft palate and secondary hard palate (Veau’s classification: Type II) (Figure 1A).
A detailed examination of the infant, followed by consultation with a prosthodontist, was carried out, and after the parents' approval, the fabrication of a feeding plate was decided on.
Fabrication of the feeding plate
Primary impression was made using low-fusing impression compound (Kerr UK Ltd,Peterborough, UK). First the defect was filled with a piece of Vaseline gauze; then green stick was softened in warm water and kneaded with caution to avoid thermal injury. An alginate spatula was used to carry the impression material into the infant’s mouth and the material was gently pressed against the hard palate and into the buccal and labial vestibules, while the baby was held in prone position in the mother’s lap. During this step the infant was crying. The impression was inspected thoroughly; it had satisfactorily covered all the supporting areas for the feeding plate (Figure 1B). Then a primary model was obtained using heavy putty rubber base (Figure 1C). The primary model was carefully inspected in order to finely determine the borders of the special tray. A 2-mm wax spacer was adapted to the primary model (Figure 2A) and the special tray was constructed with the use of a self-curing fast-setting acrylic resin (Acrostone, WHW, England; Figure 2B). The final impression was made with very high-viscosity condensation silicone rubber base impression material (ZetaplusSpA via bovazecchino, BadiaPolesine [RO], Italy), followed by light-body wash (Figure 2C).
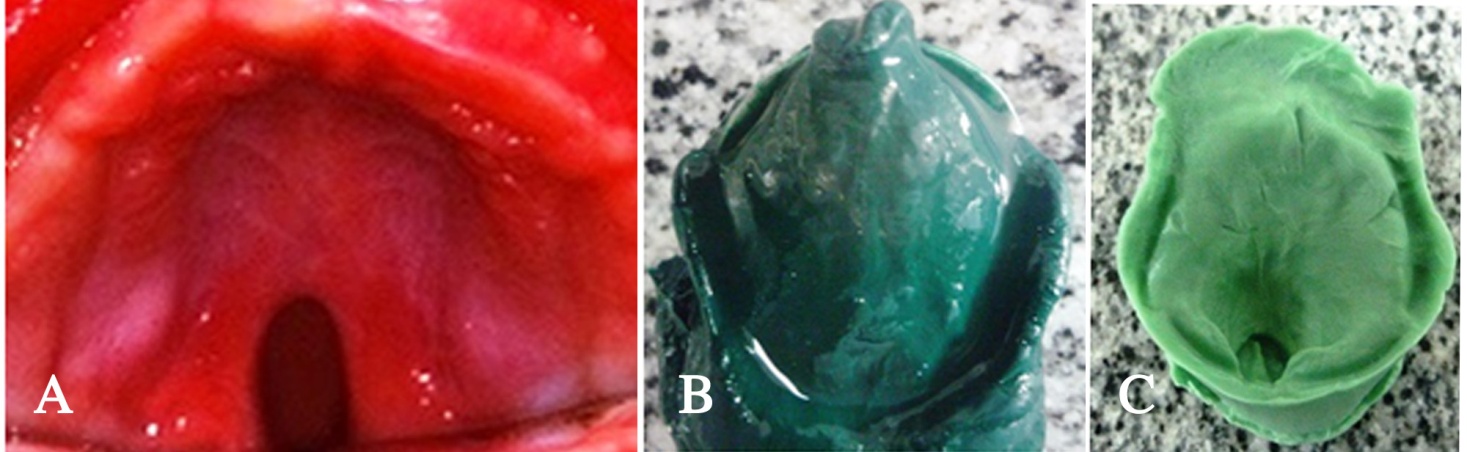
Figure 1.(A) Intraoral view of cleft palate. (B) Primary impression . (C) Primary model

Figure 2.(A) Wax spacer ,(B) Special Tray ,(C) Secondary impression, (D)Master cast
The secondary impression was poured with dental stone to obtain a master cast (Figure 2D), blocking out the undercuts with pink wax (Figure 3A); then the plate was fabricated using self-cured acrylic resin (Acrostone, WHW, England). Finally, the edges of this plate were trimmed (Figure 3B).

Figure 3.(A) Blocking undercuts , (B) Feeding plate before intraoral checking
Approximately a 10-inch silk suture (4/0 SINORGMED SILK Shandong ShengmeiMedical supplies Co.,LtD, China) was passed through and tied to the eyelet (made by small acrylic stone) of the feeding plate. The prosthesis was trimmed, finished and polished. Then it was examined in the patient’s mouth; thereafter minor adjustments and final polishing of the feeding plate were carried out (Figure 4A).

Figure 4.(A)Feeding plate after adjustment and insertion of the silk suture , (B) Intraoral view of the feeding plate
The feeding plate was checked in the dental clinic (Figure 4B) and the patient’s mother was asked to feed the baby. Instructions were provided on how to use, clean, function and maintain the feeding appliance. Monthly follow-ups were planned and the mother was informed that the feeding plate could be replaced to accommodate the craniofacial growth before surgical intervention. The infant was gained weight normally during the follow-up period.
The previously described procedure was conducted on the same day the patient was admitted into the hospital.
Discussion
The prevalence of CL/P in some Egyptian populations ranges from 0.39 to 0.51 per 1000 live births.7,8 The main objective during the first months of cleft palate infant’s life is proper weight gain, which results from proper feeding, making the infant ready for future surgical correction.5,6 Construction of a feeding appliance not only fills the gap between the nasal and oral cavities, but also it achieves maximum treatment benefits for such patients; at the same time it increases awareness and enhances the skills of diagnosis and management aspects of all the specialists in the interdisciplinary team.3,4
Making an impression is the first challenging clinical step in CP infants due to lack of cooperation on behalf of the patient. The oral cavity is too small to be adequate for commercially available impression trays, with a risk of impression material swallowing and aspiration or even being lodged in the undercuts of the defect.9,10 Therefore, it is important to take care of infant positioning, tray used and the impression material in order to maintain airway patency during impression making.
Filling the defect with a piece of Vaseline gauze helped reduce to minimum any possibilities of impression material lodgement within the defect. The impression compound was softened and placed on an alginate spatula in order to accommodate the small-sized oral cavity. Prone position was essential in keeping the tongue at forward position, avoiding posterior regurgitation of the impression material. Infant crying was satisfactory for ensuring airway patency and elimination of any possibilities of impression material aspiration. The primary impression material was poured with rubber base due to its rapid setting and since the primary cast was only used for construction of the special tray, there was no need for hard dental stone cast.
The special tray was made of self-curing acrylic resin to obtain sufficient rigidity to carry the secondary impression material. In order to obtain proper surface details, the secondary impression was taken with heavy putty type in the current case because of its high viscosity which reduces the aspiration risk. In addition, it reproduces all the areas of interest, while low-viscosity light body was used for improving details of the areas away from the defect without tearing and/or being lodged in the defect.
The final feeding plate was fabricated using fast-setting self-curing acrylic resin in an attempt to construct a single-day feeding appliance to avoid multiple visits. The plate was tied with silk to facilitate easy insertion and removal of the prosthesis and to act as a safety measure to prevent swallowing of the appliance.
The feeding plate was delivered on the same day considering high anxiety of the mother regarding the diminished weight of her infant relative to his age. The normal weight gain of the infant indicated the proper function of the feeding plate.
References
- McDonald R , A.D., Dean J., Dentistry for the child and the adolescent. . 9th ed. 2011., St. Louis:: Mosby. 614-637.
- Burg, M.L., et al., Epidemiology, Etiology, and Treatment of Isolated Cleft Palate. Front Physiol, 2016. 7: p. 67.10.3389/fphys.2016.00067.
- American Academy on Pediatric Dentistry Clinical Affairs, C. and A. American Academy on Pediatric Dentistry Council on Clinical, Policy on management of patients cleft lip/palate and other craniofacial anomalies. Pediatr Dent, 2008. 30(7 Suppl): p. 238-9.
- Association, A.C.P.C., Parameters for the Evaluation and Treatment of Patients with Cleft Lip/Palate or Other Craniofacial Anomalies. 1993; 30 (Suppl 1).revised edition 2009: Cleft Palate-Craniofacial Journal.
- Ize-Iyamu, I.N. and B.D. Saheeb, Feeding intervention in cleft lip and palate babies: a practical approach to feeding efficiency and weight gain. Int J Oral Maxillofac Surg, 2011. 40(9): p. 916-9.10.1016/j.ijom.2011.04.017.
- Duarte, G.A., R.B. Ramos, and M.C. Cardoso, Feeding methods for children with cleft lip and/or palate: a systematic review. Braz J Otorhinolaryngol, 2016. 82(5): p. 602-9.10.1016/j.bjorl.2015.10.020.
- El-Alkamy A., A.F., Elsayed H. and Hussein F., Birth prevalance of cleft lip and/or palate in Alexandria, El-Beheira, AlFayoum and Red Sea governorates. ED-Journal, 2015. 61: p. 5625.
- Balkhair M, S.S., Abd El-Sayed FA , Fahim F Birth incidence of cleft lip and/or palate in Dakahlia, Benisuif and Kafr El-sheikh governorates: a survey study. ED-Journal 2016. 62: p. 2523.
- Jones, S.D. and D.J. Drake, Case series of undetected intranasal impression material in patients with clefts. Br J Oral Maxillofac Surg, 2013. 51(3): p. e34-6.10.1016/j.bjoms.2011.11.015.
- Reichert, F., P. Amrhein, and F. Uhlemann, Unnoticed aspiration of palate plate impression material in a neonate: Diagnosis, therapy, outcome. Pediatr Pulmonol, 2017.10.1002/ppul.23710.