Comparative study of the usability of two software programs for visualization and analysis of digital orthodontic models
J Dent Res Dent Clin Dent Prospects, 12(3), 213-220; DOI:10.15171/joddd.2018.033
Original Article
Comparative study of the usability of two software programs for visualization and analysis of digital orthodontic models
Matheus Felter1,*, Milena Moraes de Oliveira Lenza2, Maurício Guilherme Lenza1, Wendel Minoro Muniz Shibazaki3, Rhonan Ferreira Silva1
1
School of Dentistry, Federal University of Goias, Goiânia, Goias, Brazil
2
Orthodontist, Master in Dentistry, Goiânia, Goias, Brazil
3
School of Dentistry, Estadual Paulista University, Araraquara, São Paulo, Brazil
*Corresponding Author ; E-mail: Paulo, contato@matheusfelter.com.br
© 2018 Felter et al. This is an Open Access article published and distributed by Tabriz University of Medical Sciences under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background
. Software programs for visualization and analysis of digital orthodontic models, apart from presenting the
necessary features for diagnosis and treatment planning, also need to be user-friendly. This characteristic refers to software’
usability, a measure that evaluates how easy it is to use it is by a specific group of professionals. The aim of this study was to
compare the usability of free available versions of two software programs for visualization and analysis of digital orthodontic
models.
Methods
. Digimodel® and OrthoCAD® usability were evaluated through their interface analysis and executing the following
procedures: malocclusion classification and models analysis (arch-length and tooth-size discrepancies).
Results
. Digimodel® and OrthoCAD® software programs had an installer only for Windows platform, occupied less than
110 megabytes of virtual space and only read files from their respective manufacturers. None possessed Portuguese as a
language option. Both allowed visualization of the models in different axes through options present in initial screen, at a click.
For model analysis, both software programs required to measure tooth to tooth and performed necessary calculations automatically.
However, OrthoCAD® software program was less intuitive because the option for these actions was among several
others, within menus, which could cause confusion during navigation. In addition, the marking of points did not always obey
the clicked site.
Conclusion
. The free access version of the evaluated software programs exhibited usability limitations related to language,
supported file format and even the model analysis execution for orthodontic diagnosis. Although OrthoCAD® was inferior,
both did not meet orthodontists’ clinical demand against these factors in the evaluated versions.
Keywords:Dental models, dental technology, orthodontics
Introduction
The representative models of dental arches were introduced to dentistry in the early 1700's and their possibility of use was improved with the development of the technique and the materials used in their preparation.1 In orthodontics, plaster models have been used for more than 100 years for diagnostic and treatment planning purposes,2 and are analyzed by orthodontists to identify and classify malocclusions,3 assess arch-length discrepancie,4,5 verify the compatibility of dental volume between the arches,6 plan and simulate mechanics indicated for dental movements in the arches (setups)7 and check the need for possible dental slices.8 Commonly, during or at the end of treatment, they are also used as reference for fabricating appliances such as orthodontic retainers, using acrylic resin.9
In addition to the clinical importance, plaster models can also be used as evidence in judicial proceedings initiated by patients,10 in cases of human identification,11 in the communication process between professionals and in the education and research sectors.1
At the end of the 1990s, digital models were introduced to orthodontics, facilitating characteristics in relation to physical plaster models, such as digital storage, speed gain and automation of dental units and interdental space measurements, and the possibility of simulation of several treatment options in the same pair of models.12
The transition from plaster to digital in orthodontics, according to the literature,13,14 is a coming reality. However, some authors15-17 consider the high cost and learning curve related to the interaction of the user with software interface as disadvantageous for their clinical use.
The use of a software program for visualization and analysis of orthodontic digital models is acceptable, like any diagnostic method, when it presents high reliability;18,19 i.e., it produces accurate results and with good agreement when applied at different moments by the same20 or by different examiners.21 Studies point to the existence of accuracy and reliability in the analysis of digital models in relation to plaster models.22,23 However, even if it possesses all the necessary features for the models analysis,24 even for clinicians who possess sufficient skill and knowledge, the software program must be accessible in terms of costs25,26 and exhibit good usability.
According to ISONORM 9241, which deals with the interaction between people and machines, usability is a measure that evaluates the ease with which a specific group of professionals can understand and perform a certain task in a computer program.27 Westerlund et al28 evaluated four software programs in orthodontics and verified that all had deficiencies in this measure, needing improvements to make the technology better and widely used by orthodontists.
Inaccurate measures taken by orthodontists for diagnostics, whether due to inability, lack of knowledge at some stage of dental treatment, or even limitations in their basic training,29 can generate clinical, ethical and legal questioning of their function,30 as the number of litigations against orthodontists have been increasing.31
In this sense, it becomes important that free software programs available for the orthodontist to visualize and analyze digital models meet usability criteria, supplying their clinical demand for diagnosis and case planning.
The aim of the present study was to compare the usability of free available versions of two software programs for visualization and analysis of digital orthodontic models (Digimodel® and OrthoCAD®).
Methods
First, software programs to be used in this paper were selected. For this purpose, a research was carried out in the literature, through Pubmed database (www.pubmed.gov.br), between 2007 and 2017, for works in which software prograsms had been used to compare measurements made in digital models with those taken in plaster models. Of 75 articles found, those with another objective were excluded. Finally, there were 16 software names in 33 papers (Table 1).
|
Table 1. Software programs found in scientific literature vs. number of papers in which they were utilized
|
|
Software program
|
Appearances
|
| OrthoAnalyzer® |
8 |
| Digimodel® |
4 |
| O3DM® |
3 |
| Rapidform® |
3 |
| BibliocastCecile3® |
2 |
| Emodel® |
2 |
| OraMetrix® |
2 |
| OrthoCAD® |
2 |
| AnatoModels® |
1 |
| Ivoris@Analyze3D® |
1 |
| MatLab® |
1 |
| Meshlab® |
1 |
| O3D® |
1 |
| Ortho3D® |
1 |
| OrthoInsight® |
1 |
| Pixform® |
1 |
The software programs were selected based on the following criteria: a) number of appearances in the literature and b) availability of a free version to download on the manufacturer's website. This way, Digimodel® (OrthoProof, New Mexico, USA) and OrthoCAD® (Align Technology, San Jose, California, USA) software programs were selected for comparison because, based on the two established criteria, these were the first ones matching them. However, with fewer appearances than other software programs, at the time of this survey (August 2017), OrthoCAD® was the software program, found by researchers, as the second option that provided a free version available for use.
The two selected software programs were then downloaded to a personal computer, along with sample models provided by the manufacturers and analyzed separately. Software usability analysis was performed by checking, mainly, the following items:
-
Type of installer
-
Virtual space required to install the program
-
File formats supported by the program
-
Languages available for navigation
-
Possibility of classifying malocclusion in digital models
-
Possibility of performing model analysis (arch-length and tooth-size discrepancies)
Data were annotated and the interfaces were compared and discussed according to possible advantages or disadvantages related to them.
Results
Digimodel® and OrthoCAD® software programs had an installer only for Windows platform, occupied less than 110 megabytes of virtual space each and only read files from their respective manufacturers. Both presented icons as action buttons to assist in the users’ orientation for a more intuitive navigation, and none of them possessed Portuguese as a language option.
Only OrthoCAD® allowed saving measurements or tasks that were performed in a session of use of the program to continue later. In addition, it also allowed the export of images of the work screen in JPEG format, unlike Digimodel®, which had export options in HTML and TXT format, but blocked in the evaluated version (Table 2).
|
Software programs’ technical information
|
|
Digimodel®
|
OrthoCAD®
|
|
CHARACTERISTICS
|
|
|
| Installer platform |
Windows |
Windows |
| Virtual space |
22 megabytes |
107 megabytes |
| Supported file format |
Manufacturer’s only (.opds) |
Manufacturer’s only (.3dm) |
| Language |
English |
English/Russian |
Available features
|
- Marking of points to perform measurements (option available on the software’s initial screen, described as "measurements");
- Visualization of the upper and lower models, separated or occluded, in different views, by means of a click, in the software initial screen;
- Possibility to visualize models in order to establish malocclusion classification;
- Automatic calculation of overjet and overbite in two clicks (no need of marking points for these tasks);
- Individual tooth-length measurements and annotations (3 clicks: 1 for tooth selection, and 2 for marking points);
- Automatic calculations of arch-length and tooth-size discrepancies (it is needed that teeth dimensions are already marked). |
- Marking of points to perform measurements (option available after opening a “Diagnostic” menu and clicking the “measurements” option within it);
- Visualization of the upper and lower models, separated or occluded, in different views, by means of a click, in the software initial screen;
- Possibility to visualize models in order to establish malocclusion classification;
- Automatic calculation of overjet and overbite in two clicks (no need of marking points for these tasks);
- Individual tooth-length measurements and annotations (3 clicks: 1 for tooth selection, and 2 for marking points);
- Automatic calculation of arch-length and tooth-size discrepancies (it is needed that teeth dimensions are already marked);
- Automatic calculations for Korkhaus analysis;
- Possibility to save the work done to continue later;
- Possibility to export screenshots in JPEG format. |
Both software programs allowed the visualization of the models in different axes in just one click through options present in the initial screen (Figures 1 and 2), which permitted and facilitated the task of classifying malocclusion.
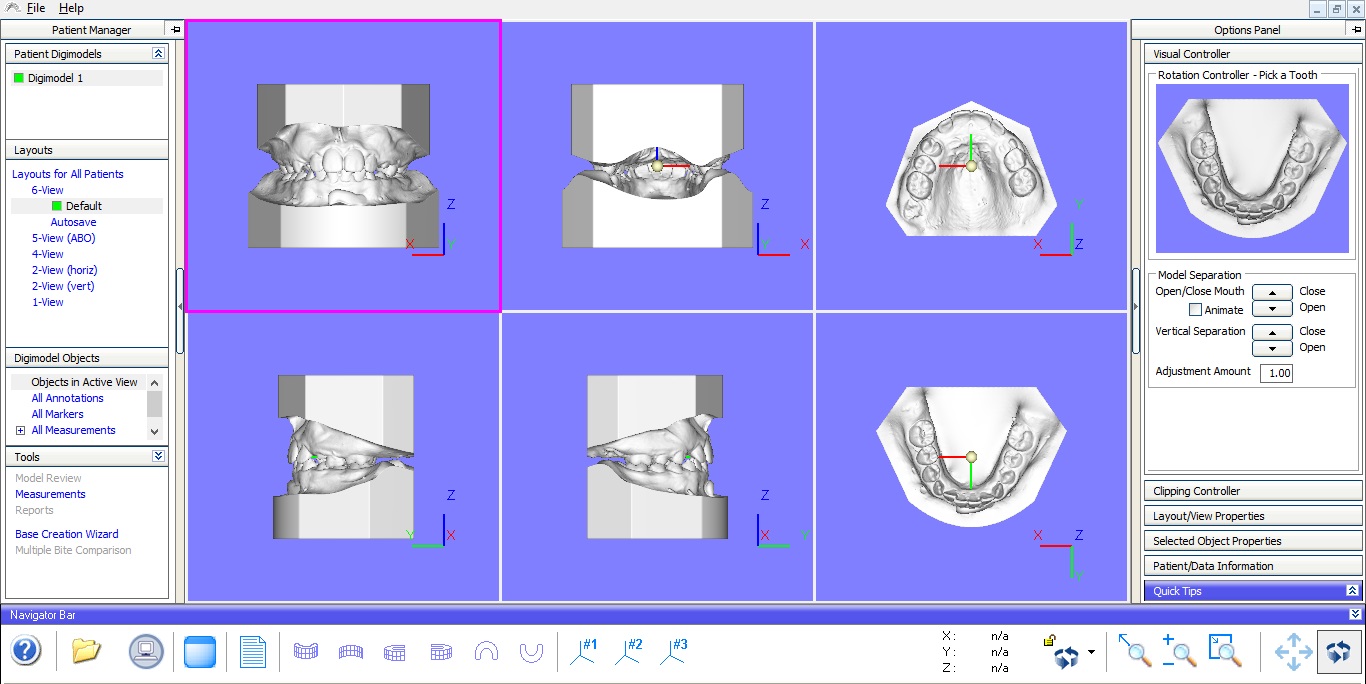
Digimodel® software program interface.
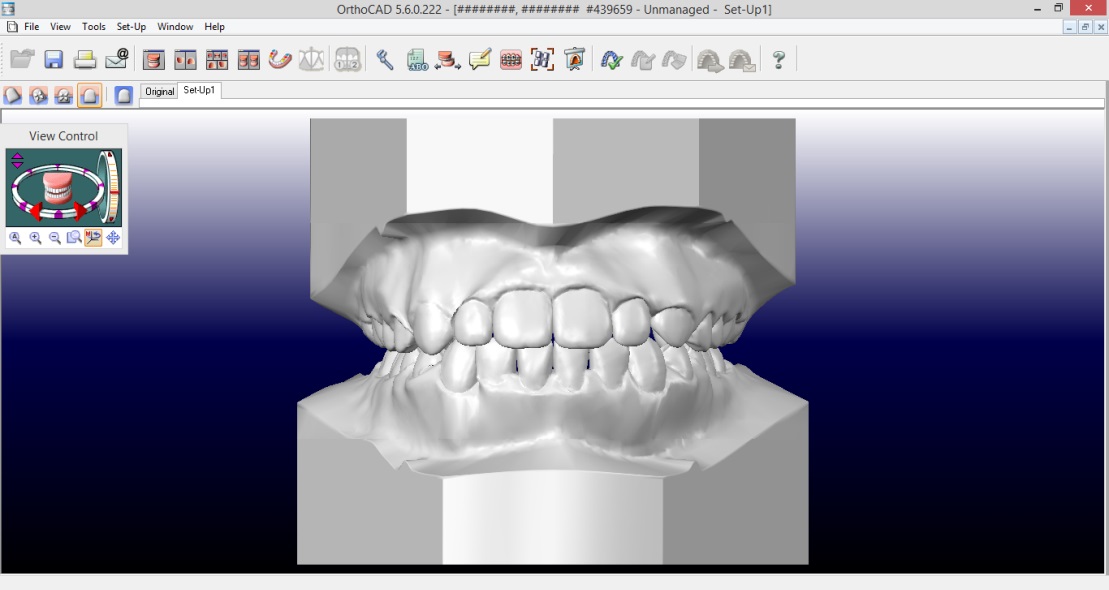
OrthoCAD® software program interface.
In models analysis, both software programs required tooth-to-tooth measurements and performed calculations of each analysis automatically, presenting them in a separate window (Figures 3 and 4).
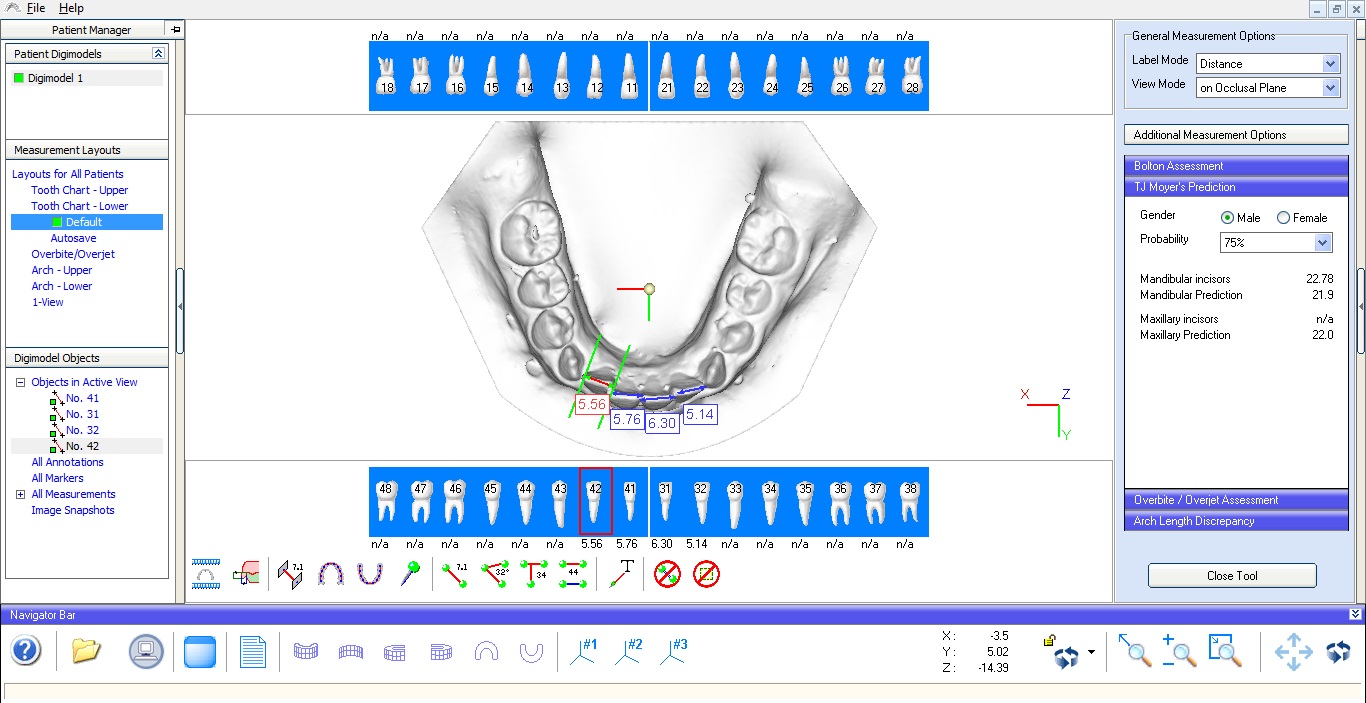
Tooth measurements taken in Digimodel® software program.
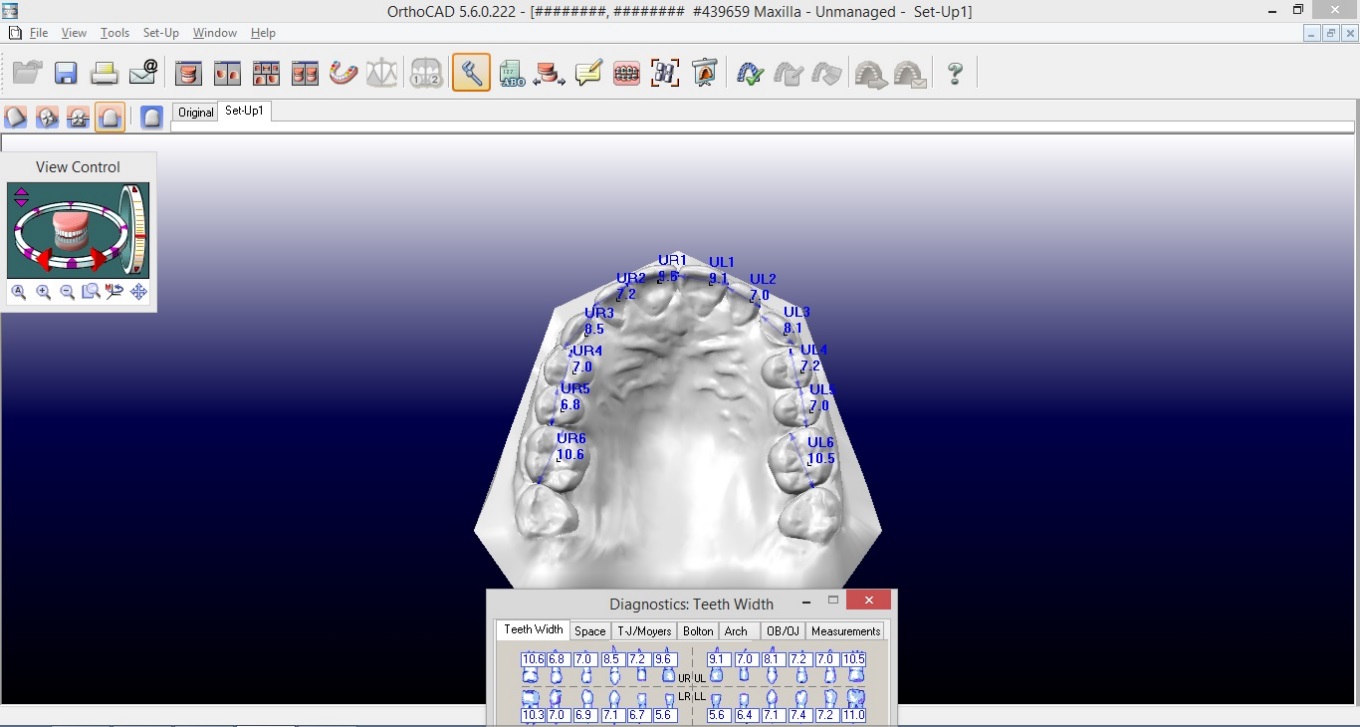
Tooth measurements taken in OrthoCAD® software program.
Discussion
The software progrsams Digimodel® and OrthoCAD® automate the calculations necessary to perform two important analyses for orthodontic diagnosis (bone‒dental discrepancy and inter-arch dental volume compatibility), as well as facilitate the classification of malocclusions through rapid access to different view axes/angles necessary for this task.
The accuracy, precision and reliability of Digimodel®33,34 and OrthoCAD®35,36 have been demonstrated in other studies. However, studies on the usability of this type of software program are still extremely scarce.28 In addition, the lack of standardization in the scientific term used to find articles on usability,37 as well as the unavailability of the Portuguese language in software, are barriers that may hinder advances in Brazilian orthodontics in this area, depriving many orthodontists who do not speak English of using this technology.
The concept of usability, brought by the ISONORM 9241, points to it as a measure that evaluates the ease with which a specific group of professionals can understand and perform a certain task in a computer program.27 In view of this, the usability of the OrthoCAD® software can be considered inferior to that of the Digimodel® software program due to its complexity in finding the tools (options) that allow actions common to the use of orthodontists.3-6 This reduced usability of OrthoCAD® software program compared to Digimodel® software program, which can be attributed to two factors: a) the amount of functionality offered generates more confusion during navigation in the software program, demotivating users to understand and use it;38 b) the marking of points to measure distances does not always obey the clicked site on the screen. This is consistent with Westerlund et al,28 who considered the usability of OrthoCAD® and three other software programs as weak. Digimodel® was not one of them. However, if it were included in these authors' paper, it would probably also be considered weak if evaluated by the same criteria that they used.
The methodology of the present work sought to evaluate free access versions of the most researched software programs in the literature in order to verify if their use could be wider, considering their ease of use and availability of necessary tools for orthodontic diagnosis. However, as found by Hassan et al,16 it was verified that the software programs evaluated in the present study allowed to work only with files in their own format. This means that the universal file format for orthodontic digital models (STL) is not downloadable in these software programs, making it possible, for the time being, to use them mainly in foreign countries due to patents in Digital Dentistry.
OrthoCAD® software program, for example, is available since 199917 when it was launched in the market and is the most widely used orthodontic digital visualization and analysis software program in graduate programs in orthodontics in Canada and the United States.32 Although it has several potential benefits for its users,12 its free access version does not make its usufruct possible in locations that have scanning systems capable of producing only digital models in their standard format. The evaluated version of Digimodel® software program also had this same limitation.
Considering that the free access versions of the software programs evaluated meet the important criterion of being accessible in terms of cost,25,26 the factors discussed so far demonstrate that although they present several important functionalities for orthodontic diagnosis and treatment planning, they also have limitations when it comes to meet the demand of the Brazilian orthodontists who work with generic manufacturers' scanners, which are usually more accessible to them.
It should be remembered that digital models allow, in addition to the advantages related to the clinical workflow itself, the reduction of the need for physical space for model keeping, as it happens in the case of plaster models.12 Therefore, it would be advantageous for Brazilian orthodontists since the small physical space of their offices could be used for purposes other than archiving objects that occupy significant volumes in cabinets or shelves. T
his issue must also be considered from the ethical and legal points of view. Law cases against orthodontists have increased in numbers over time, both abroad31and in Brazil.39
The Brazilian Code of Ethical Dentistry40 recommends that the professional must file patient documentation, which includes their models, for an indefinite period.41 On the other hand, from the legal point of view, it is also important that models be stored because they can be used in civil cases in which there is allegation of possible dental error.42 Under Brazilian civil law, according to Law 13.105, of March 2015, in its articles 369, 422 and 441, it is not impeditive to the digital documents (among them the models) as legal proofs, since it is provided from a suitable source.43 In addition, the digital format for orthodontic models, which make the measurement of teeth in the arches possible, allows them to be used for expert purposes if necessary, such as human identification, limited in some cases to examination of dental information of the probable victim.44 In this context, with the guarding of patient models becoming unavoidable, its digital version would make it easier to comply with such ethical issues and to protect dental professionals in possible conflicts with patients.
Although the present study has focused on issues related to diagnosis and treatment planning, it should be remembered that orthodontic treatment itself also brings with it undesirable side effects, such as tooth enamel wear and patient hygiene difficulties.45,46 Ways to control them, even in the details of each procedure, can help the clinician beware of possible litigation.
Conclusion
The free access versions of the evaluated software programs present usability limitations related to the language and the supported file format. Although OrthoCAD® and Digimodel® present important functionalities for orthodontic diagnosis and treatment planning, the first one may have a barrier to learning or adoption by professionals in face of their variety of functions and difficulty in marking points, while the other cannot allow continuity in the workflow or data export.
Authors’ contributions
WMMS and RFS contributed to the concept and design. MF contributed to data acquisition, analysis and interpretation. MMOL contributed to data interpretation and revision of its intellectual content. MGL contributed to data interpretation and revision of its intellectual content. All authors have read and approved the final manuscript.
Ethical issues
Not applicable.
References
- Peluso MJ, Josell SD, Levine SW, Lorei BJ. Digital models: An introduction. Seminars in Orthodontics2004;10(3):226–38.doi: https://doi.org/10.1053/j.sodo.2004.05.007. [Crossref]
- Angle EH. Bone growing. Dent cosmos 1910;52:261–7.
- Angle EH. Classification of malocclusion. Dent cosmos 1899;41(3):248–64.
- Little RM. The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod Dentofacial Orthop 1975;68(5):554–63.
- Philip NI, Prabhakar M, Arora D, Chopra S. Applicability of the Moyers mixed dentition probability tables and new prediction aids for a contemporary population in India. Am J Orthod Dentofacial Orthop 2010;138(3):339–45.doi: 10.1016/j.ajodo.2008.09.035. [Crossref]
- Bolton WA. The clinical application of a tooth-size analysis. Am J Orthod Dentofacial Orthop1962;48(7):504–29.
- Vianna MS, Saga AY, Casagrande FA, Carmargo ES. Setup: um auxílio no diagnóstico ortodôntico. J Bras Ortodon Facial 2002;7(41):398-405.
- Cuoghi OA, Sella RC, Macedo FA, Mendonça MR. Desgaste interproximal e suas implicações clínicas. J Dental Press Ortodon Ortop Facial 2007;12(3):32-46.doi: 10.1590/S1415-54192007000300005. [Crossref]
- Pithon MM, Lacerda-Santos R, Soares N, Fogaça DNL, da Silva WS, Rodrigues LB et al. Influence of the manipulation technique of acrylic resin on mechanical strength of orthodontic plates. Biosci J 2015;31(6).doi: 10.14393/BJ-v31n6a2015-29095. [Crossref]
- Paranhos LR, Magalhães MPM, Francio J, Terada HH, Rosário HD, Silva RF. Tempo de guarda da documentação ortodôntica versus prazo de prescrição legal. Dental Press J Orthod 2013;18(3):113-7.
- Paranhos LR, Caldas JFC, Iwashita AR, Scanavini MA, Júnior ED. A importância da documentação ortodôntica nas perícias de identificação humana. Ortodontia 2008;41(esp):297-301.
- Fleming PS, Marinho V, Johal A. Orthodontic measurements on digital study models compared with plaster models: a systematic review. Orthodontics & Craniofacial Research 2011;14(1):1–16. doi: 10.1111/j.1601-6343.2010.01503.x. [Crossref]
- Zimmermann M, Mehl A, Mormann WH, Reich S. Intraoral scanning systems – a current overview. International Journal of Computerized Dentistry 2015;18(2): 101-129.
- Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi L. Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: a systematic review. AJODO 2016;149(2).doi: 10.1016/j.ajodo.2015.06.029. [Crossref]
- Santoro M, Galkin S, Teredesai M, Nicolay OF, Cangialosi TJ. Comparison of measurements made on digital and plaster models. Am J Orthod Dentofacial Orthop 2003;124(1):101–5. doi: 10.1016/S0889540603001525. [Crossref]
- Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S. Evaluation of the accuracy of digital model analysis for the American Board of Orthodontics objective grading system for dental casts. Am J Orthod Dentofacial Orthop 2005;128(5):624–9. doi: 10.1016/j.ajodo.2004.08.017. [Crossref]
- Stevens DR, Flores-Mir C, Nebbe B, Raboud DW, Heo G, Major PW. Validity, reliability, and reproducibility of plaster vs digital study models: Comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am J Orthod Dentofacial Orthop 2006;129(6):794–803. doi: 10.1016/j.ajodo.2004.08.023. [Crossref]
- Brandão MM, Sobral MC, Vogel CJ. Reliability of Bolton analysis evaluation in tridimensional virtual models. Dental Press J Orthod 2015;20(5):72-7.doi: 10.1590/2177-6709.20.5.072-077.oar. [Crossref]
- Pithon MM, Lacerda-Santos R, Araújo JTS, Coqueiro RS. Applicability of moyers' probability table in the population of the northeast of brazil. Biosci J 2015;31(1). doi: 10.14393/BJ-v31n1a2015-26073. [Crossref]
- Lemos LS, Rebello IMCR, Vogel CJ, Barbosa MC. Realiability of measurements made on scanned cast models using the 3Shape R700 scanner. Dentomaxillofac Radiol 2014;44.doi: 10.1259/dmfr.20140337. [Crossref]
- Fabels LNJ, Nijkamp PG. Interexaminer and intraexaminer reliabitilies of 3-dimensional orthodontic digital setups. AJODO 2014;146(6).doi: 10.1016/j.ajodo.2014.09.008. [Crossref]
- Kim J, Heo G, Lagravère MO. Accuracy of laser-scanner models compared to plaster models and cone-beam computed tomography. Angle Orthodontist 2014;84(3).doi: 10.2319/051213-365.1. [Crossref]
- Rosseto MC, Palma FMC, Ferreira RI, Pinzan A, Vellini-Ferreira F. Comparative study of dental arch width in plaster models, fotocopies and digitized images. Braz Oral Res 2009;23(2):190-5.
- Moreira T, Urzal V, Correia A, Ferreira AP. Contributo para a caracterização da Ortodontia Portuguesa considerando a utilização de recursos informáticos. Rev Por Estomatol Med Dent Cir Maxilofac 2012;53(1):17-23.doi: https://doi.org/10.1016/j.rpemd.2011.11.003. [Crossref]
- Sollenius O, Petrén S, Bjornsson L, Norlund A, Bondmark L. Health economic evaluations in orthodontics: a systematic review. Eur J Orthodon 2016;38(3):259-265.doi: 10.1093/ejo/cjv040. [Crossref]
- Chun JS, Har A, Lim HP, Lim HJ. The analysis of cost-effectiveness of implant and conventional fixed dental prosthesis. J Adv Prosthodont 2016;8:53-61.doi: 10.4047/jap.2016.8.1.53. [Crossref]
- ISO CD 9241-11: Ergonomics of human-system interactions – Part 11: usability: definitions and concepts.
- Westerlund A, Tancredi W, Ransjo M, Bresin A, Psonis S & Torgersson O. Digital cast in orthodontics: a comparison of 4 software systems. Am J Orthod Dentofacial Orthop 2015; 147:509-16.doi: 10.1016/j.ajodo.2014.11.020. [Crossref]
- Brandão AMM, Brandão GAM, Jesus AS, Flório FM. Profile of orthodontic education in brazilian undergraduate dentistry courses. Biosci J 2017;33(2):555-565. doi: 10.14393/BJ-v33n2-34878. [Crossref]
- Barreto GM, Feitosa HO. Iatrogenics in Orthodontics and its challenges. Dental Press J Orthod 2016;21(5):114-25.doi: 10.1590/2177-6709.21.5.114-125.sar. [Crossref]
- Mizrahi E. Risk management in clinical practice. Part 7. Dento-legal aspects of orthodontic practice. British Dental Journal 2010;209(8).doi: 10.1038/sj.bdj.2010.926. [Crossref]
- Shastry S, Park JH. Evaluation of the use of digital study models in postgraduate orthodontic programs in the United States and Canada. Angle Orthod 2014;84(1):62-67.doi: 10.2319/030813-197.1. [Crossref]
- White AJ, Fallis DW, Vanderwalle KD. Analysis of intra-arch and interarch measurements from digital models with 2 impression materials and a modeling process based on cone-beam computed tomography 2010;137(4):456.e1-456.e9.doi: 10.1016/j.ajodo.2009.09.019. [Crossref]
- Naidu D, Scott J, Ong D, Ho CTC. Validity, reliability and reproducibility of three methods used to measure tooth widths for Bolton analysis. Austr Orthod 2009;25(2):97-103.
- Naidu D, Freer TJ. Validity, reliability and reproducibility of the iOC intraoral scanner: a comparison of tooth widths and Bolton ratios. Am J Orthod Dentofacial Orthop 2013;144:304-310.doi: dx.doi.org/10.1016/j.ajodo.2013.04.011. [Crossref]
- Leifert MF, Leifert MM, Efstratiadis SS, Cangialosi TJ. Comparison of space analysis evalutions with digital models and plaster dental casts. Am J Orthod Dentofacial Orthop 2009;136:16.e1-16.e4.doi: 10.1016/j.ajodo.2008.11.019. [Crossref]
- Weinerth K, Koenig V, Brunner M, Martin R. Concept maps: a useful and usable tool for computed-based knowledge assessment? A literature review with focus in usability. Computers & Education 2014;78:201-209. doi: https://doi.org/10.1016/j.compedu.2014.06.002. [Crossref]
- Iyengar SS, Lepper MR. When choice is demotivating: can one desire too much of a good thing? Journal of Personality and Social Psychology 2000;79(6):995-1006.
- Barbosa ACF, Barbosa MJL, Marchiori GE, Mendes TE, Paranhos LR. Decisões dos tribunais quanto à obrigação dos profissionais da ortodontia: uma revisão de 10 anos. Biosci J 2013;29(5):1388-1394.
- Brasil. Conselho Federal de Odontologia. Código de Ética Odontológica. Aprovado pela Resolução CFO-118/2012. 2013. Disponível em: http://cfo.org.br/wpcontent/uploads/2009/09/codigo_etica.pdf.
- Paranhos LR, Magalhães MPM, Francio J, Terada HH, Rosário HD, Silva RF. Time of guard of orthodontic records versus legal time for their prescription. Dental Press J. Orthod 2013;18(3):113-117. doi: 10.1590/S2176-94512013000300018. [Crossref]
- Ramos DIA, Daruge Júnior E, Daruge E, Antunes CM, Meléndez BVC, Francesquini Júnior L et al. Transposición dental y sus implicaciones éticas e legales. Revista ADM 2005;62(5):185-190.
- Brasil. Lei nº 13.105, de 16 de março de 2015. Código do Processo Civil. Disponível em: http://www.planalto.gov.br/ccivil_03/_ato2015-2018/2015/lei/l13105.htm. Acesso em 20 de março de 2018.
- Silva RF, Chaves P, Paranhos LR, Lenza MA, Daruge Júnior E. Use of orthodontic records in human identification 2011;16(2):52-57. doi: 10.1590/S2176-94512011000200007. [Crossref]
- Ferreira EF, Vilani GNL, Jansen WC, Brito HHA, Ferreira RAN, Manzi FR et al. Enamel loss and superficial aspect during bonding and debonding of metallic brackets 2016;32(2):550-559. doi: 10.14393/BJ-v32n2a2016-30162. [Crossref]
- Pithon MM, Sant’Anna LIDA, Baião FCS, Coqueiro RS, Maia LC, Paranhos LR. Effectiveness of different mechanical bacterial plaque removal methods in patients with fixed orthodontic appliance: a systematic review and meta-analysis. Biosci J 2017;33(2):537-554.