Restoring a
post-traumatic partial edentulous mandible with the Toronto prosthesis: a
clinical report
J Dent Res Dent Clin Dent Prospects, 12(2), 135-139; DOI:10.15171/joddd.2018.021
Clinical Dentistry
Restoring a
post-traumatic partial edentulous mandible with the Toronto prosthesis: a
clinical report
Fatemeh Nematollahi1, Marzieh Alikhasi2, Elaheh Beyabanaki 3*
1
Department of Prosthodontics, Islamic Azad University, Dental Branch, Tehran, Iran
2
Dental Implant Research Center and Department of Prosthodontics, Tehran University of Medical Sciences, School of Dentistry, Tehran, Iran
3
Department of Prosthodontics, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
*Corresponding Author; Email: e.beyabanaki@gmail.com
© 2018 by Tabriz University of Medical Sciences
Abstract
Implants
provide support, stability and retention for restorations used in fully and
partially edentulous patients. This clinical report describes prosthetic
treatment of a 30-year-old man suffering from a dentoalveolar deficiency due
to an old gunshot trauma to the left side of the mandible. The patient was rehabilitated
with implant-supported Toronto prosthesis following surgical placement of
three implants with undesirable location and angulations due to lack of
sufficient bone. This prosthetic option offers advantages of both
screw-retained and cement-retained prostheses and provides acceptable
aesthetic and functional results.
Keywords: Dental cement, dental implant, implant-supported dental prosthesis
Introduction
There are some critical factors for long-term success of dental implants, such as bone quality, position of implants1-3 and superstructure design in order to equally distribute occlusal loads among the implants.4-6 Although avoiding misaligned implants would help provide the patient with favorable esthetic and functional results, this is not always possible.7,8 There are some factors that inhibit augmentation of resorbed or defective alveolar ridges prior to implant placement, including surgical cost or patient health-related problems.9,10 Therefore it is expected that prosthetic restoration of mouth would also be complicated.
Generally there are two types of fixed implant-supported prostheses: screw-retained and cement-retained prostheses. Screw-retained restorations provide ease of retrievability of restoration for repair, hygiene measurements or retightening of abutment screw.11 However, this option may produce complications regarding location of screw access hole for misaligned implants, in terms of esthetic and occlusion.12 Moreover, if the metal framework design does not support the porcelain around the access hole, it might lead to porcelain fracture in this area.13
On the other hand, cement-retained restorations present several advantages over screw-retained restorations. These benefits include ease of fabrication, being aesthetically pleasing, simpler placement in posterior regions of the oral cavity and higher potential for achieving passive fit in the superstructure.14,15 However, they have some disadvantages such as difficulty in removing the restoration and remaining of cement excess around the implant.16
Toronto bridge technique17 or abutment-hybrid overdenture18 has been suggested in order to overcome problems of both types of aforementioned restorations and yet benefiting from their merits. In this technique the substructure is a screw-retained framework on which individual crowns would be cemented and pink or gingiva-colored porcelain or laboratory composite is used for mimicking the soft tissues.16-20 Rajan and Gunaseelan21 first described fabricating retrievable cement-retained and screw-retained implant prosthesis for single-tooth implant-supported restorations. This prosthesis offers the advantages of both cement-retained and screw-retained restorations such as retrievability of the abutment and the prosthesis, and easy removal of the prosthesis for cleaning the excess cement. The aim of this article was to present a case treated with Toronto prosthesis for restoration of partial edentulism in a post-traumatic mandible.
Clinical Report
A 30-year-old partially edentulous patient was referred to the Implant Department of Tehran University, School of Dentistry, for prosthetic reconstruction (Figure 1, a and b). The patient had lost 6 teeth due to the trauma of a gunshot. Since the accident had occurred several years prevoiusly and the patient had undergone cosmetic plastic surgery, only a skin scar remained in his lower face. Three implants (Implantium, Dentium, Seoul, South Korea) were placed on the left side of the mandible (Figure 2, a and b). Regarding the increased interocclusal space and improper implant alignment, it was decided to use hybrid screw-retained and cement-retained implant (Toronto) prosthesis.
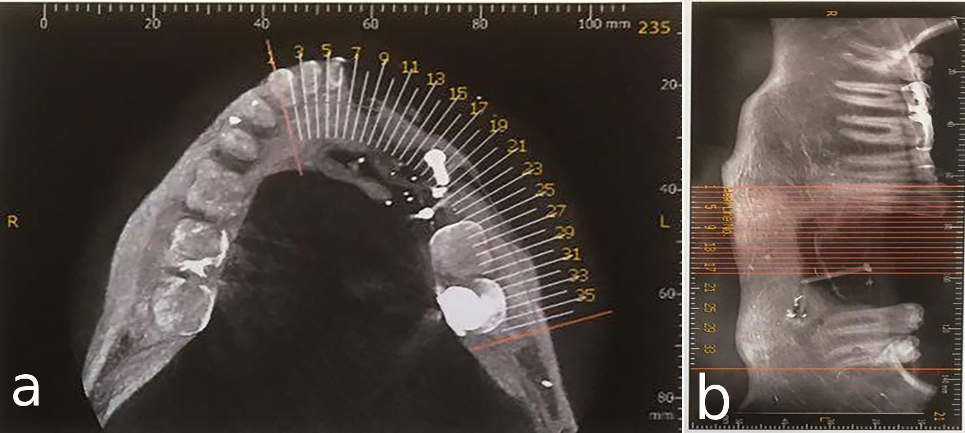
a) Occlusal view of the mandible after gunshot injury. b) Side view of the left side of the mandible after gunshot injury
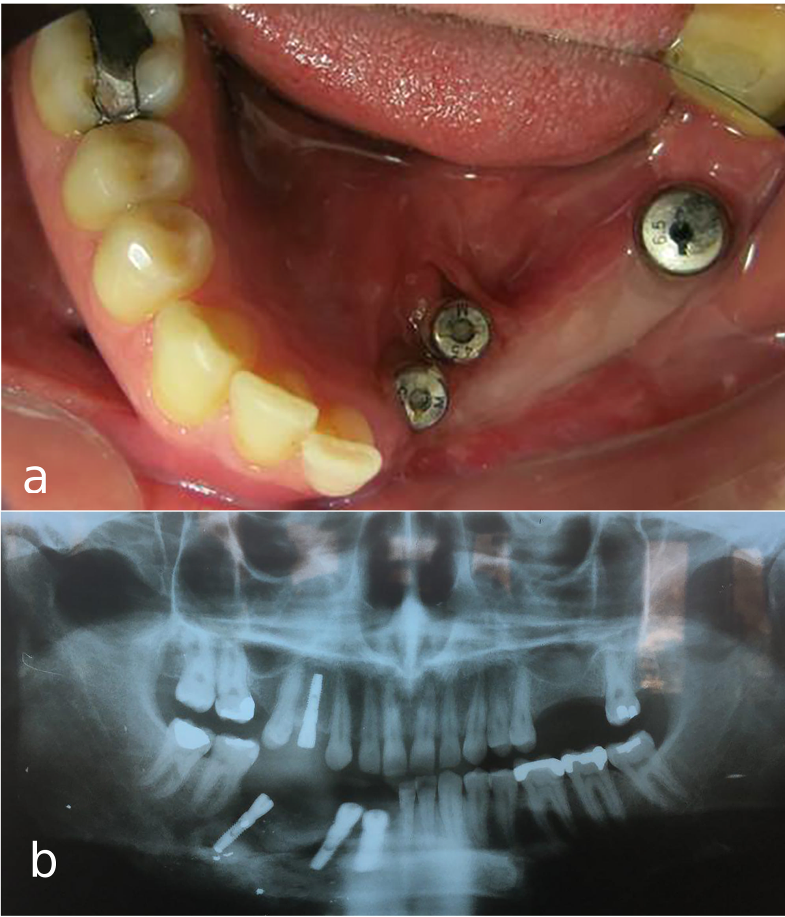
a) Occlusal view of mandibular arch with three implants. b) Panoramic view of implants placed in defective bone in the left mandible.
Using auto-polymerizing acrylic resin (Pattern Resin, GC, Tokyo, Japan) square impression copings were splinted, and an open-tray implant-level impression was made with polyvinyl siloxane impression material (Monopren Transfer, Kettenbach GmbH& Co., KG, Germany).22 Also, an irreversible hydrocolloid impression (Alginoplast; Heraeus Kulzer, Hanau, Germany) was made of the upper jaw. After attaching implant analogs to the impression copings in the impression, a silicone material (GI mask; Coltene/Whaledent, Cuyahoga Falls, Ohio) was injected around the coping analogs to serve as gingival tissues around the implants. Then, type IV dental stone (Hero Stone Vigodent Inc; Rio de Janeiro – Brazil) was used for pouring the impressions.
To record the jaw relationship, a screw-retained record base was made on the master cast. Before making the jaw relationship record, the occlusal surface of maxillary second premolar was reduced about 1 mm using a football-shaped diamond finishing bur (Tizkavan, Iran) to address its minimal supraeruption. After recording the centric position of the mandible with lower record base and occlusion rim opposing the upper teeth, using an inter-occlusal registration material (Virtual; IvoclarVivadent, Schaan, Liechtenstein), the casts were mounted in a semi-adjustable articulator (Dentatus ARH, Stockholm, Sweden) using a facebow transfer record. Then, acrylic denture teeth (Apple, Ideal Maco, Tehran, Iran) were set up on the record base and tried in the patient mouth for evaluation of tooth arrangement, position, length, gingival level and contour. Subsequently, a silicone (Panasil, Kettenbach GmbH& Co., KG, Germany) index was fabricated of the approved tooth set-up on the record base.
After connecting plastic abutments (burn-out sleeve) (Implantium, Dentium) to the implant analogs on the master cast with 10 N/cm torque, the acrylic resin (Pattern Resin, GC, Tokyo, Japan) pattern of infrastructure (meso-structure) was made using previously made silicone index as the guide (Figure 3, a). The pattern was then cut back in order to produce cores in the form of prepared teeth, and also to provide room for gingiva-colored porcelain replacing soft and hard tissue support. The resin pattern of the framework was tried in the oral cavity to verify the accuracy of impression procedure before casting (Figure 3, b). The passive fit of the cast framework with multiple individual abutments was confirmed in the oral cavity by means of one-screw test and periapical radiographs (Figure 4).5,6
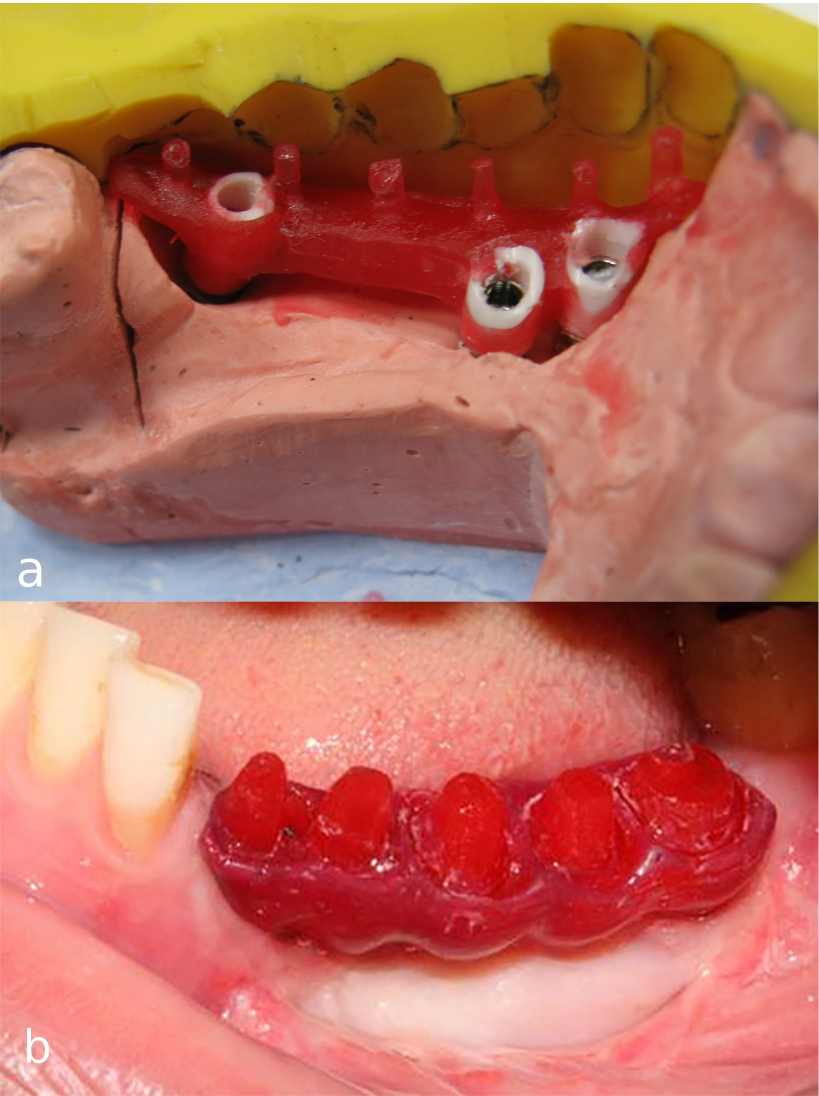
a) Fabrication of acrylic resin pattern of framework using plastic abutments. b) Try-in of the acrylic resin framework.

Try-in of the metal framework.
Subsequently, gingiva-colored porcelain was baked on the gingival part of the framework by the aid of silicone index for controlling the gingival contour. After evaluating gingival adaptation of the framework intraorally (Figure 5), the copings of the superstructure (crowns) were directly waxed up on the framework. The fit of metal-ceramic crowns was assessed in the patient's oral cavity afterwards. Group function occlusion was created on the left working side to distribute functional loads on all the three implants.

Try-in of metal framework with gingiva-colored porcelain.
Finally after screwing the meso-structure with 30 N/cm torque according to manufacturer’s instructions, Teflon tape (SITCO, Fujian China) was placed at the orifice of screw holes and covered with light-cured composite resin. Finally, the crowns were cemented with temporary cement (Temp-Bond, Kerr, Italy) on the metal framework (Figure 6).

Delivery of prosthesis with cemented individual crowns.
Discussion
The patient presented in this report was treated with a hybrid cement-retained and screw-retained implant restoration. This kind of restoration is mainly indicated for demanding esthetic situations, excessive inter-occlusal space, and when vertical bone augmentation is not feasible.16 This kind of prosthesis could be used for restoring a single tooth,21 or partial16,19 and even a full18,20 edentulous arch. The main advantage of this kind of restoration is that not only implant position or angulation would not affect the design of the substructure, but also implant emergences could be corrected.18 Considering severe misalignment of the middle implant due to insufficient bone volume in the canine site as a result of an old gunshot injury in this case, this prosthetic option was selected. Also, regardless of location of screw access holes in the meso-structure, each crown can be fabricated in a position which is esthetically and functionally desirable.,17 Furthermore, when a great amount of porcelain is fired on the metal framework in cases of increased inter-occlusal space, distortion of the framework and loss of passive fit is expected. However, Toronto bridge technique prevents such distortion and also enables the possibility of replacing a damaged crown without jeopardizing the fit of the framework by re-firing it.16-20 Another advantage of this technique is that the esthetic and occlusion concerns usually seen in screw-retained restorations due to screw access hole are overcome.17,18 Moreover, retrievability of crowns cemented with temporary cement makes their maintenance relatively easy.16-20
However, the disadvantages entitled to this technique are difficulty of adjusting the crown's contact points, probability of crown dislodgement due to the use of a temporary cement, difficulty of achieving passive fit of screw-retained framework and high cost.17-19
This technique offers some varieties in terms of material used for framework, including casting,21 zirconia19 and CAD-CAM milled titanium20 frameworks. Also, gingiva-colored composite resin16 could be used for covering the gingival part of the framework.
Authors’ contributions
All authors contributed to the case selection, and treatment planning. FN, MA, and EB contributed to the treatment of the patient. FN and EB together drafted the manuscript. All authors have contributed to the critical revision of the manuscript, and have read and approved the final manuscript.
Competing interests
The authors declare no competing interests with regards to the authorship and/or publication of this article.
Ethics approval
The individual whose information is included in the report has given written informed consent for the publication of this paper.
References
- Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications with implants and implant prostheses. J Prosthet Dent 2003;90(2):121-32. DOI:10.1016/S0022-3913(03)00212-9. [Crossref]
- Lemmerman KJ, Lemmerman NE. Osseointegrated dental implants in private practice: a long-term case series study. J Periodontol 2005;76(2):310-9. DOI:10.1902/jop.2005.76.2.310. [Crossref]
- Kan JY, Rungcharassaeng K, Bohsali K, Goodacre CJ, Lang BR. Clinical methods for evaluating implant framework fit. J Prosthet Dent 1999;81(1):7-13.
- Kim Y, Oh TJ, Misch CE, Wang HL. Occlusal considerations in implant therapy: clinical guidelines with biomechanical rationale. Clin Oral Implants Res 2005;16(1):26-35. DOI:10.1111/j.1600-0501.2004.01067.x. [Crossref]
- Tan KB, Rubenstein JE, Nicholls JI, Yuodelies RA. Three dimentional analysis of the casting of the casting accuracy of one piece, osseointegrated implant retained prostheses. Int J Prosthodont 1993; 6(4): 346 – 63.
- Papaspyridakos P, Hirayama H, Chen CJ, Ho CH, Chronopoulos V, Weber HP. Full-arch implant fixed prostheses: a comparative study on the effect of connection type and impression technique on accuracy of fit. Clin Oral Implants Res. 2016; 27(9):1099-105. doi: 10.1111/clr.12695. [Crossref]
- Kopp KC, Koslow AH, Abdo OS. Predictable implant placement with a diagnostic/surgical template and advanced radiographic imaging. J Prosthet Dent 2003;89(6):611-5. DOI:10.1016/S0022391303001987. [Crossref]
- Minoretti R, Merz BR, Triaca A. Predetermined implant positioning by means of a novel guide template technique. Clin Oral Implants Res 2000;11(3):266-72.
- Balshi TJ. Preventing and resolving complications with osseointegrated implants. Dent Clin North Am 1989;33(4):821-68.
- Strietzel FP. Patient’s informed consent prior to implant-prosthetic treatment: a retrospective analysis of expert opinions. Int J Oral Maxillofac Implants 2003;18(3):433-9.
- Nissan J, Narobai D, Gross O, Ghelfan O, Chaushu G. Long-term outcome of cemented versus screw-retained implant-supported partial restorations. Int J Oral Maxillofac Implants 2011;26(5):1102–7.
- Chee W, Felton DA, Johnson PF, Sullivan DY. Cemented versus screw-retained implant prostheses: which is better? Int J Oral Maxillofac Implants 1999;14(1):137–41.
- Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant restorations: achieving optimal occlusion and esthetics in implant dentistry. J Prosthet Dent 1997;77(1):28–35.
- Michalakis KX, Hirayama H, Garefis PD. Cement-retained versus screw-retained implant restorations: a critical review. Int J Oral Maxillofac Implants 2003;18(5):719–28.
- Karl M, Taylor TD, Wichmann MG, Heckmann SM. In vivo stress behavior in cemented and screw-retained five-unit implant FPDs. J Prosthodont 2006;15(1):20–4.
- Hagiwara Y, Nakajima K, Tsuge T, McGlumphy EA. The use of customized implant frameworks with gingival-colored composite resin to restore deficient gingival architecture. J Prosthet Dent 2007;97(2):112–7. DOI:10.1016/j.prosdent.2006.12.011. [Crossref]
- Cicciù M, Risitano G, Maiorana C, Franceschini G. Parametric analysis of the strength in the ''Toronto'' osseous-prosthesis system. Minerva Stomatol 2009;58 (1-2):9–23.
- Montero J, Macedo de Paula C, Albaladejo A.The "Toronto prosthesis", an appealing method for restoring patients candidates for hybrid overdentures: A case report. J Clin Exp Dent. 2012 ;4 (5):309-12. doi: 10.4317/jced.50877. [Crossref]
- Uludag B, Ozturk O, Celik G, Goktug G. Fabrication of a retrievable cement- and screw-retained implant-supported zirconium fixed partial denture: a case report. J Oral Implantol 2008;34(1):59–62. doi: 10.1563/1548-1336(2008)34[59:FOARCA]2.0.CO;2. [Crossref]
- Baig MR, Rajan G, Rajan M. Edentulous arch treatment with a CAD/CAM screw-retained.
- framework and cemented crowns: a clinical case report. J Oral Implantol 2009;35(5):295-9. doi: 10.1563/AAID-JOI-D-09-00012R1.1. [Crossref]
- Rajan M, Gunaseelan R. Fabrication of a cement and screwretained implant prosthesis. J Prosthet Dent 2004;92(6):578–80. doi:10.1016/S0022391304006092. [Crossref]
- Beyabanaki E, Shamshiri AR, Alikhasi M, Monzavi A. Effect of Splinting on Dimensional Accuracy of Impressions Made of Implants with Different Subgingival Alignments. J Prosthodont. 2017 ;26(1):48-55. doi: 10.1111/jopr.1236. [Crossref]